Introduction
According to the National Alliance of State Pharmacy Associations (NASPA) and the American Pharmacists Association (APhA), only 19 states and Washington, DC, allow pharmacists, independently or by protocol, to administer all Advisory Committee on Immunization Practices (ACIP) recommended vaccines to individuals aged 3 and older, including some with no minimum age requirement (National Alliance of State Pharmacy Associations, 2025). Pharmacists are increasingly recognized as key providers of pediatric immunizations due to their accessibility, expertise, and community presence. Studies show that pharmacist-administered pediatric vaccines improve access and uptake, especially in underserved and rural areas, without delaying preventive care like well-child visits (Bhardwaj et al., 2025; Daniel et al., 2021). Parents express strong support for pharmacy-based vaccination, and research confirms that pharmacies can successfully serve as Vaccines for Children providers, improving HPV and COVID-19 vaccination rates among children and adolescents (Calo et al., 2019; Daniel et al., 2021; Kim et al., 2022). Expanding pharmacist authority can close coverage gaps, reduce missed opportunities, and strengthen public health preparedness (Bhardwaj et al., 2025; Kim et al., 2022).
Pharmacists are key contributors to expanding immunization efforts by offering accessible vaccination services for both adult and pediatric populations. Their ability to provide vaccines outside of traditional healthcare settings coupled with extended operating hours makes pharmacists uniquely positioned to reduce barriers to care, especially for patients with limited access to primary care providers (Goad et al., 2013). Training requirements for pharmacists to administer immunizations include education and training on hands-on deltoid intramuscular and subcutaneous injection techniques, clinical assessment, and emergency reaction management (American Pharmacists Association, 2026). The Centers for Disease Control and Prevention (CDC) recommends deltoid administration of vaccines for all individuals older than three years of age, reducing vaccination administration complexity and requirements for additional training in comparison to children younger than three, where administration is in the thigh (Centers for Disease Control and Prevention, 2026a). Despite pharmacist authority to administer childhood vaccinations and similarities between vaccine administration of adults and children, differences exist in the percentage of adult and pediatric vaccines administered at pharmacies, with limited data analyzing this discrepancy. While the proportion of adult vaccines administered at pharmacies has steadily increased over the past decade, data show that pediatric vaccination rates lag, raising questions about barriers specific to pharmacy-based pediatric immunization services (Centers for Disease Control and Prevention, 2026b; Kim et al., 2022).
Several barriers impede the delivery of pharmacy-based pediatric immunizations, including systemic, provider, and patient-related factors. Many parents are hesitant to have their children vaccinated at pharmacies due to unfamiliarity with pharmacists’ roles in healthcare and concerns about vaccine availability and training standards (Calo et al., 2019; Omecene et al., 2019; Teeter et al., 2021). Pediatric patients may also experience heightened injection-related anxiety and stress, which may be exacerbated by the lack of private spaces in pharmacies for vaccine administration (Teeter et al., 2021). Systemic obstacles include limited insurance coverage for pharmacy-administered pediatric vaccines and cumbersome requirements for pharmacy enrollment in programs like Vaccines for Children (VFC) which restrict access for Medicaid participants and create financial disincentives for pharmacies (Calo et al., 2019; Daniel et al., 2021). Additionally, some physicians have expressed concerns about reduced follow-up opportunities and inaccurate vaccine records when children are vaccinated outside of traditional settings which may further complicate collaboration between pharmacies and physician offices (Omecene et al., 2019; Shah, Calo, et al., 2018; Shah, Marciniak, et al., 2018). Strategies such as improving the public awareness of pharmacists’ qualifications, streamlining vaccine reimbursement processes, and strengthening physician-pharmacist partnerships could help overcome these barriers and improve pediatric immunization rates. This study aims to characterize pharmacy-based immunizers’ comfort levels with administering pediatric vaccines in community pharmacy settings and to identify perceived barriers that may limit their participation in pediatric immunization efforts. Specifically, this study seeks to inform educational and training strategies and to identify workflow and system-level factors that may influence pharmacist engagement in pediatric vaccination.
This study addresses an important gap in the literature, as prior research has primarily focused on access and outcomes of pharmacy-based vaccination, with limited data describing provider-level comfort across pediatric age groups and the specific barriers influencing these differences. The factors explored in this study, such as experience, training, anatomical considerations, and behavioral challenges, align with established behavioral frameworks (e.g., the Capability, Opportunity, Motivation–Behavior [COM-B] model) (Michie et al., 2011), where provider capability (skills and training) and opportunity (practice environment and workflow) may influence vaccination behaviors. While this study was not explicitly designed using a behavioral framework, these constructs provide a useful lens for interpreting pharmacist participation in pediatric immunization.
Methods
This study was an institutional review board (IRB) approved, cross-sectional convenience survey designed to assess the comfort level of community pharmacy-based immunizers in administering vaccines to pediatric patients aged 3 to 18 years. The study population included California pharmacists, student pharmacists, and pharmacy technicians actively administering vaccines in California community pharmacy settings. Individuals were excluded if they had not administered a vaccine in the past five years, were not licensed in California, did not practice in a community setting or did not consent to the survey. The survey was conducted using Qualtrics® (Provo, UT) and distributed electronically via professional pharmacy organizations and pharmacy school mailing lists in California between November 2022 and February 2023. Participation was voluntary, anonymous, and the survey was administered in English.
The survey collected demographic information and assessed participants’ comfort level in administering vaccines to patients in five age categories: less than 3 years, 3–4 years, 5–10 years, 11–17 years, and 18 years or older. Comfort level was measured on a four-point Likert scale, with response options of extremely comfortable, somewhat comfortable, somewhat uncomfortable, and extremely uncomfortable. Participants also selected from perceived barriers to pediatric vaccine administration, which included anatomical challenges, behavioral factors, parental concerns, training deficits, and experience. Additionally, the survey gathered data on the average number of pediatric vaccines administered per week and ranked administered pediatric vaccines from most to least common.
Data analysis was performed using descriptive and inferential statistics. Fisher’s exact test was used to determine statistical significance in responses between pharmacists and student pharmacists and between age groups. All statistical analyses were conducted using RStudio (version 2022.12.0+353). Proportional differences between student pharmacists and pharmacists and between different ages of patients were compared using Fisher’s exact test. Statistics were performed using The R Project software version 4.4.2 using an RStudio graphical user interface.
Results
From November 2022 - February 2023, 178 participants (105 student pharmacists; 73 pharmacists) met inclusion criteria. The two groups were similar with respect to baseline characteristics. Due to the small sample size (n=5), technicians were not included in the analysis. A full breakdown of the characteristics of respondents is included in table 1.
For ease of analysis, responses of “extremely comfortable” and “somewhat comfortable” were combined into a single “comfortable” category, while “somewhat uncomfortable” and “extremely uncomfortable” were grouped as “uncomfortable.” The number of participants indicating they were uncomfortable administering vaccines to adults was negligible and thus excluded from analysis. No significant differences were found between student pharmacists and pharmacists in feeling comfortable delivering vaccines to any of the age groups <3 years, 3-4 years, 5-10 years, or 11-17 years (p=0.3922, p=0.163, p=0.3981, and p=1 respectively), thus these two groups were collapsed into one group of 153 participants for subsequent analysis.
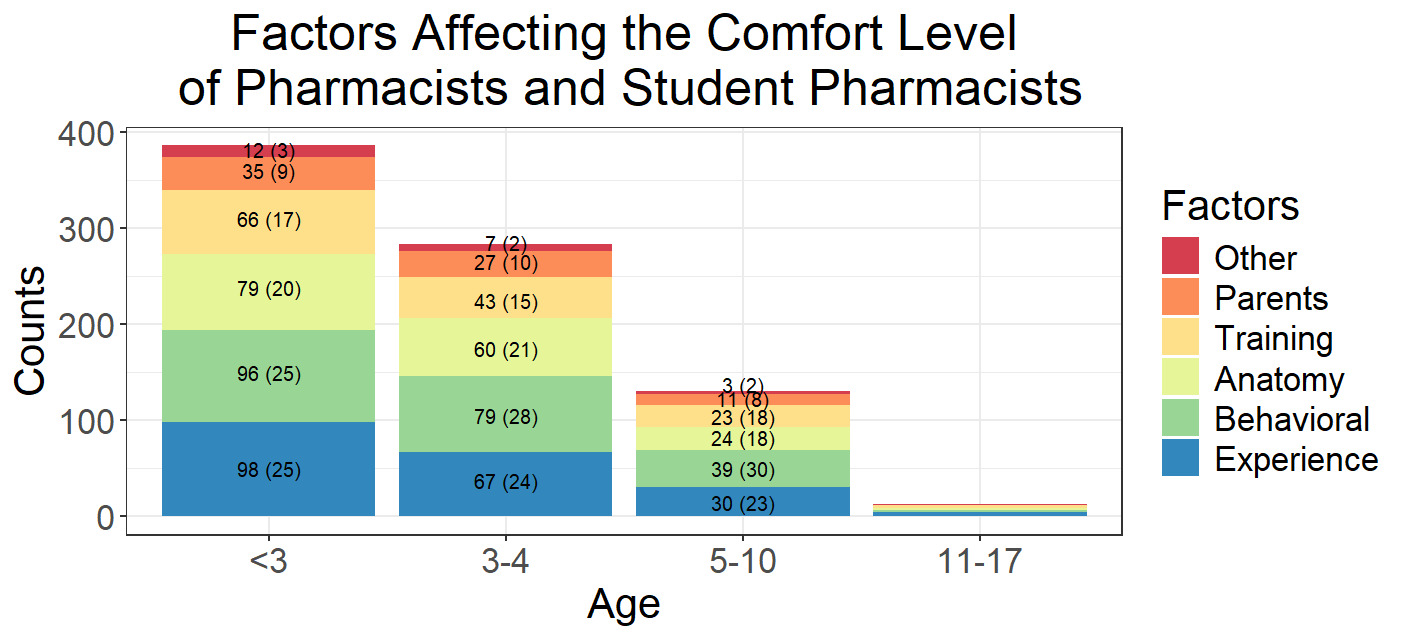
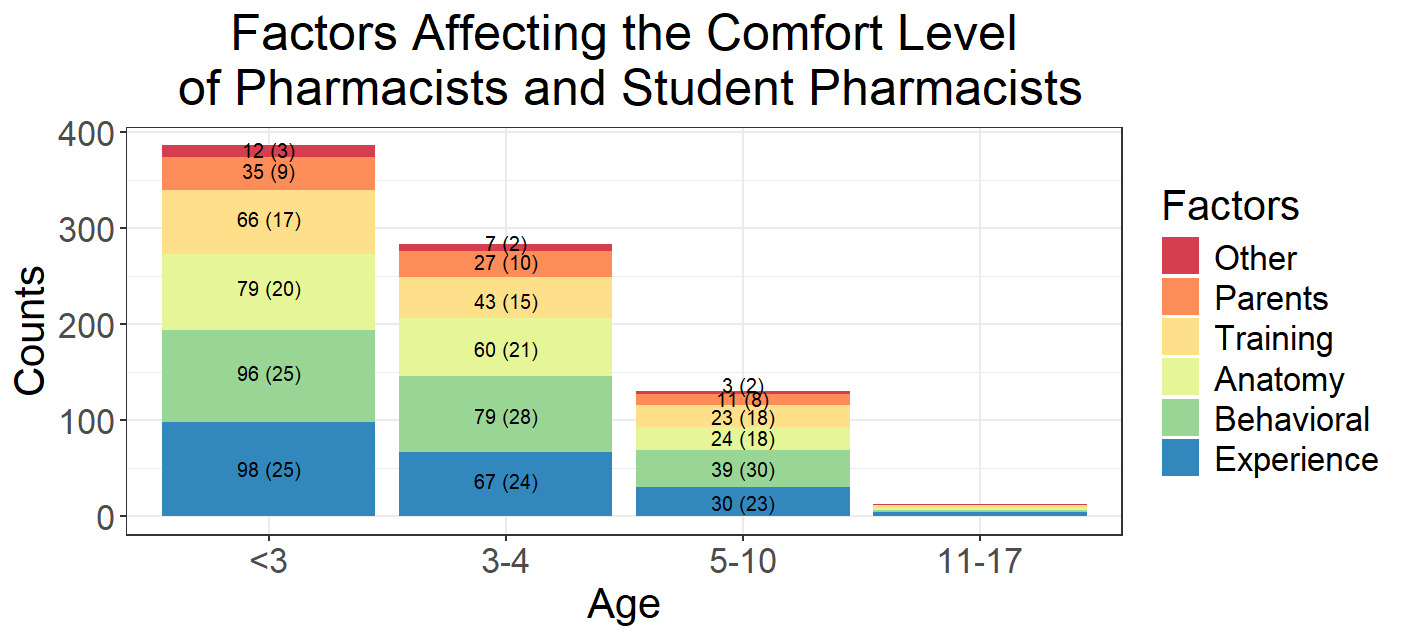
There were, however, statistically significant differences in the comfort level between the different age groups (p < 0.01 for all comparisons). Our subjects were 1.42 times more likely to be comfortable vaccinating 3-4 year olds as compared to children under 3, 1.74 times more likely to be comfortable vaccinating 5-10 year olds as compared to 3-4 year olds, and 5.02 times more likely to be comfortable vaccinating 11-17 year olds as compared to 5-10 year olds, see table 2 for a full breakdown. The most common factors that impacted comfort were behavioral issues with the child (83% across all age groups), lack of experience (72% for all age groups), anatomical challenges (51% for all age groups), lack of training (50% for all age groups), and parental influence (27%) (see Figure 1). There were two free responses not covered in the existing choices, which were a lack of access to medical records and a lack of time to administer to children. The top 5 most common vaccines administered by pharmacy-based immunizers to children less than 18 years of age (in order) were influenza, COVID-19, Tdap, PCV, and MMR. Free responses from survey respondents who said they received training vaccinating children less than 3 years of age, cited multiple sources, including formal educational programs, workplace training, and independent learning. Many participants completed training through CDC resources, including CDC immunization training videos and continuing education (CE) courses. The APhA immunization training program, corporate-sponsored computer-based training, and the Pharmacist Letter were also cited as key educational resources. Workplace training was also reported, particularly focusing on injection techniques using the vastus lateralis of young children. Some respondents received hands-on guidance from registered nurses (RNs) or physicians, who helped them refine their vaccination techniques and ensure proper muscle identification. Additional specialized training was obtained through the fire department and a school of pharmacy-based mobile vaccination program.
Discussion
To our knowledge, this is the first study of its kind to describe the comfort levels of pharmacy-based immunizers when vaccinating pediatric patients across different age groups. During the COVID-19 pandemic, significant gaps in pediatric vaccinations started occurring as ACIP routinely recommended vaccination rates significantly dropped due to providers delaying routine in person visits for children (Santoli et al., 2020). In the initial phase of the pandemic, many primary care providers, clinics, and hospitals prioritized acute care services, shifting vaccination services to community pharmacies which reinforced the importance of the community pharmacy as a vaccination destination (AlMahasis et al., 2023). Overall, pharmacists administered more than 200 million COVID-19 vaccines from 2020 to 2022 (Grabenstein, 2022). For pediatric patients in need of COVID-19 vaccines, parents accepted pharmacy-based immunizers as 46.4% of vaccines were administered in this setting. However, this acceptance rate did not extend to the administration of routine pediatric immunizations as only 12.3% of influenza vaccinations were administered in community pharmacies as compared to physician offices where 66.7% of seasonal influenza vaccines were administered during the pandemic (Centers for Disease Control and Prevention, 2026b). One explanation for this may be the concern that pediatric patients who receive routine vaccines in community pharmacies may have delayed or missed well-child visits since most children receive these vaccines in primary care settings. However, a recent study illustrated that there were no statistically significant differences in having a timely well child visit between children who received vaccines in pharmacies and those who received them in a primary care setting (Bhardwaj et al., 2025).
The findings of this study can be interpreted within a behavioral framework in which provider participation in pediatric vaccination is influenced by both capability and opportunity. Barriers identified in this study, such as lack of experience, limited training, anatomical challenges, and difficulty managing pediatric patient behavior, primarily reflect limitations in capability, while factors such as workflow constraints, staffing limitations, and practice environment may represent opportunity-related barriers (Michie et al., 2011). Although these constructs were not directly measured, this framework provides a useful structure for understanding how these factors may collectively influence pharmacist engagement in pediatric immunization.
Pharmacist involvement in vaccination efforts greatly increases patient access and accessibility to this public health service (Berenbrok et al., 2022). Pharmacist involvement has also been shown to build trust within communities as evidenced by previous studies showing pharmacists play a positive role in improving vaccination rates, patient/parent awareness, and vaccination hesitancy (Bach & Goad, 2015; Le et al., 2022). Student pharmacists are also able to vaccinate after successful completion of a training program approved by the Accreditation Council for Pharmacy Education (ACPE), such as the APhA Pharmacy-Based Immunization Delivery Training Program while being supervised by a licensed and immunization certified pharmacist. The positive effects stemming from pharmacist provided vaccination services along with the ability of student pharmacists to vaccinate under pharmacist supervision greatly helps to address pediatric vaccination barriers by ensuring increased accessibility, higher vaccination rates, and improved patient outcomes.
This potential, however, may be tempered by a lack of pharmacist comfort to safely immunize the pediatric population as identified in the present study where both pharmacists and student pharmacists were shown to be less comfortable vaccinating patients ten years of age and under compared to children eleven years of age and up. Our data indicates that while experience vaccinating children less than 3 years old and the child’s behavior were equivalent, the child’s behavior becomes the most common factor affecting comfort level for children 3 to 10 years of age. The behavioral issues during the vaccination process are likely due to immunization stress-related responses (ISRRs) such as crying, combativeness, and hyperactivity; injection fears; and acute anxiety often exacerbated by the lack of private vaccination rooms (Teeter et al., 2021). These ISRRs can also pose challenges for vaccinators as identified in the present study and can result in lower vaccination rates. Patients experiencing ISRRs may require additional support which may be unavailable in the community pharmacy setting as pharmacists are usually the sole healthcare professional present with limited assistance (Omecene et al., 2019). As a result, physician offices are often perceived as safer vaccination locations (Shah, Calo, et al., 2018; Shah, Marciniak, et al., 2018). In addition to individual-level factors, structural and workflow-related barriers likely contribute to these challenges. Community pharmacy settings may lack private space, sufficient staffing, or time required to manage pediatric patients experiencing anxiety or stress-related responses, which may further limit pharmacists’ willingness to vaccinate younger children.
To increase pediatric vaccination rates, raising pharmacist and student pharmacist comfort levels needs to be addressed. This could be supported by additional training in pediatric vaccinations, which has been associated with improving both pharmacists’ and student pharmacists’ confidence and comfort with administering and counseling on vaccines for the adolescent population (McCauley et al., 2020). This training needs to specifically include injection into the vastus lateralis muscle (i.e. thigh muscle), recommended for children under 3 years of age, as the current APhA program only trains on deltoid muscle administration and the subcutaneous route. While many pharmacy schools already integrate the APhA Immunization Certificate Training Program into their curricula, the incorporation of pediatric vaccination training does not appear to be widespread (Phan et al., 2025; Prescott & Bernhardi, 2019). However, when such training has been incorporated, student’s perceived knowledge and confidence in providing pediatric vaccinations has been shown to increase (Miller et al., 2022). Interestingly, while participants in this study reported receiving pediatric vaccination training, the current APhA Immunization Certificate Training Program only offers an optional supplementary module on pediatric vaccination which does not include a hands-on practicum. Our findings, however, reinforce the importance of ensuring that pharmacists and student pharmacists are adequately trained to vaccinate patients of all age groups. Handling behavioral responses of the child, learning the correct anatomical placement of vaccines, and addressing parental concerns during the vaccination process are all topics that should be included in standardized vaccination training programs. While direct evidence linking training to increased vaccination rates is limited, expanding training opportunities can help address competency gaps and may contribute to higher pediatric vaccination rates by improving comfort levels. These findings suggest that targeted educational interventions, particularly those focused on pediatric-specific injection technique, behavioral management, and anatomical considerations, may help address capability-related barriers identified in this study.
These findings have important implications for pharmacy education, practice, and policy. From an educational perspective, incorporating hands-on pediatric vaccination training, simulation-based learning, and behavioral management strategies into pharmacy curricula and continuing education programs may help improve provider comfort. From a practice standpoint, addressing workflow constraints, staffing support, and physical space considerations may enhance the feasibility of pediatric vaccination in community pharmacies. At the policy level, reducing administrative barriers such as Vaccines for Children program participation and reimbursement limitations may further encourage pharmacist involvement in pediatric immunization services.
This study has several limitations that should be considered when interpreting the findings. The cross-sectional design limits the ability to infer causal relationships between pharmacy-based immunizer comfort levels and barriers to pediatric vaccine administration. Longitudinal studies are therefore needed to assess how comfort levels evolve with training and experience over time. Selection bias may have also influenced the results of this study as survey data is from a small convenience sample of respondents. California has over 50,000 licensed pharmacists and about 5,000 intern (student) pharmacists, with a greater proportion of student representation in this study sample. However, it is difficult to fully describe the impact of this as students have fewer years of practice experience, but all are trained to immunize, which may not be the case with all practicing community pharmacists. There is no officially published data on the breakdown of pharmacists by practice setting in California, but national data suggests that approximately 59% practice in community settings, with 10.7% in independent, and 41% in chain settings (Mott et al., 2024). Our sample was slightly skewed toward independent at 40%, with chain at 35%. Further, the survey was distributed electronically through professional pharmacy organizations and pharmacy school mailing lists, which may have led to the overrepresentation of individuals already engaged in professional development or those with a particular interest in immunization services. As a result, we were unable to determine a response rate and were prevented from assessing nonresponse bias. Insufficient responses to demographic questions limited the analysis of their impact on pharmacist and student pharmacist comfort. Lastly, this study was conducted in California where pharmacy-based immunization laws may differ from those in other states, territories, or countries. The generalizability of the findings may therefore be limited, particularly in regions with different regulatory environments, training requirements, or parental perceptions of pharmacist-administered vaccinations.
Conclusions
This study highlights the varying comfort levels of pharmacy-based immunizers in administering pediatric vaccines and the potential barriers that may hinder their participation in childhood immunization efforts. Despite pharmacists’ expanding role in vaccine administration in California, challenges such as lack of experience, training, different anatomical sites for administration, parental hesitancy, and dealing with young child behavior during vaccination persist. Addressing these barriers through targeted education, training, and policy initiatives could enhance pharmacist confidence and increase pediatric vaccination uptake in community pharmacies. Future research should focus on evaluating effective strategies, including training resources and educational materials, to support pharmacists in overcoming these challenges and ensuring equitable vaccine access for pediatric populations.
Author Contributions
conceptualization: JG, KH, LB RB; methodology: JG, KH, LB RB; formal analysis: JG, RB; Investigation: JG, KH, LB; writing – original draft: JG, KH, LB RB; writing – reviewing and editing: JG, KH, LB RB; supervision: JG; funding acquisition: n/a
Funding, Conflicts of Interest
The authors report that no funding was requested or utilized to prepare this manuscript or honorarium received for and have no conflicts of interest to report.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Chapman University (protocol code IRB 23-94, approved 11/10/22)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors wish to acknowledge the 2022-23 Chapman University School of Pharmacy Student Leadership Team (Nikki Derleth, Paolo Tristian Domingo, Anabelle Gantman, Elyn Lam, Brian Le, Rosa Le, Inna Marie Tagarino, Helen Vu) for their initial research on this subject which lead to the creation of this manuscript.